Trachoom


De Lairessestraat 59 1071 NT Amsterdam 020-679 71 55 omca@me.com www.omca.nl
Trachoom (conjunctivitis granulosa, ophthalmia aegyptica) is een langdurige infectie van het bindvlies die door de bacterie Chlamydia trachomatisserotype A-C wordt veroorzaakt.
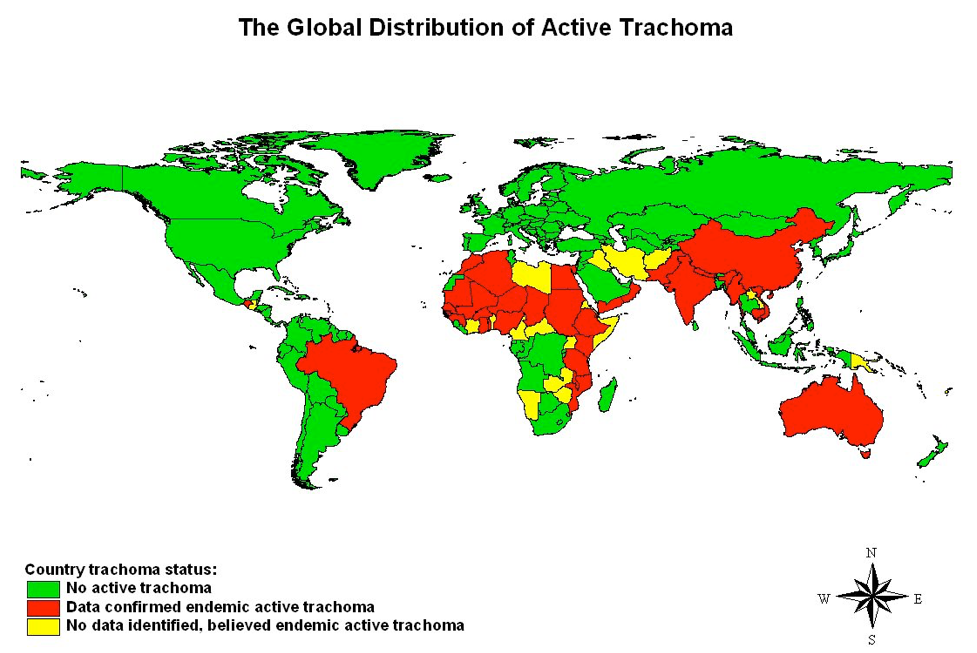
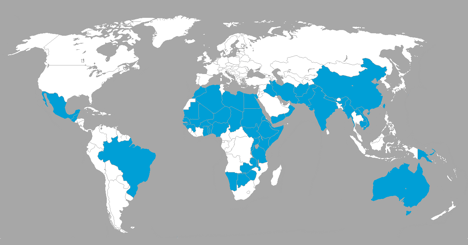
Trachoom is wereldwijd de belangrijkste te voorkomen oorzaak van blindheid en is het gevolg van chronische of herhaalde infecties met bepaalde niet-seksueel overgedragen stammen van Chlamydia trachomatis. Trachoom komt veel voor in armere streken in de droge, warme landen in Noord-Afrika, het Midden-Oosten, India en Zuidoost-Azië.
In Nederland en België komt trachoom zelden voor, hoewel het soms optreedt onder immigranten afkomstig uit gebieden waar trachoom wel vaak voorkomt.
De ziekte komt het meeste voor bij kinderen, vooral tussen de 3 en 6 jaar oud. Oudere kinderen en volwassenen hebben een veel kleiner risico om de ziekte te krijgen omdat zij beter immuun zijn en een betere persoonlijke hygiëne hebben.
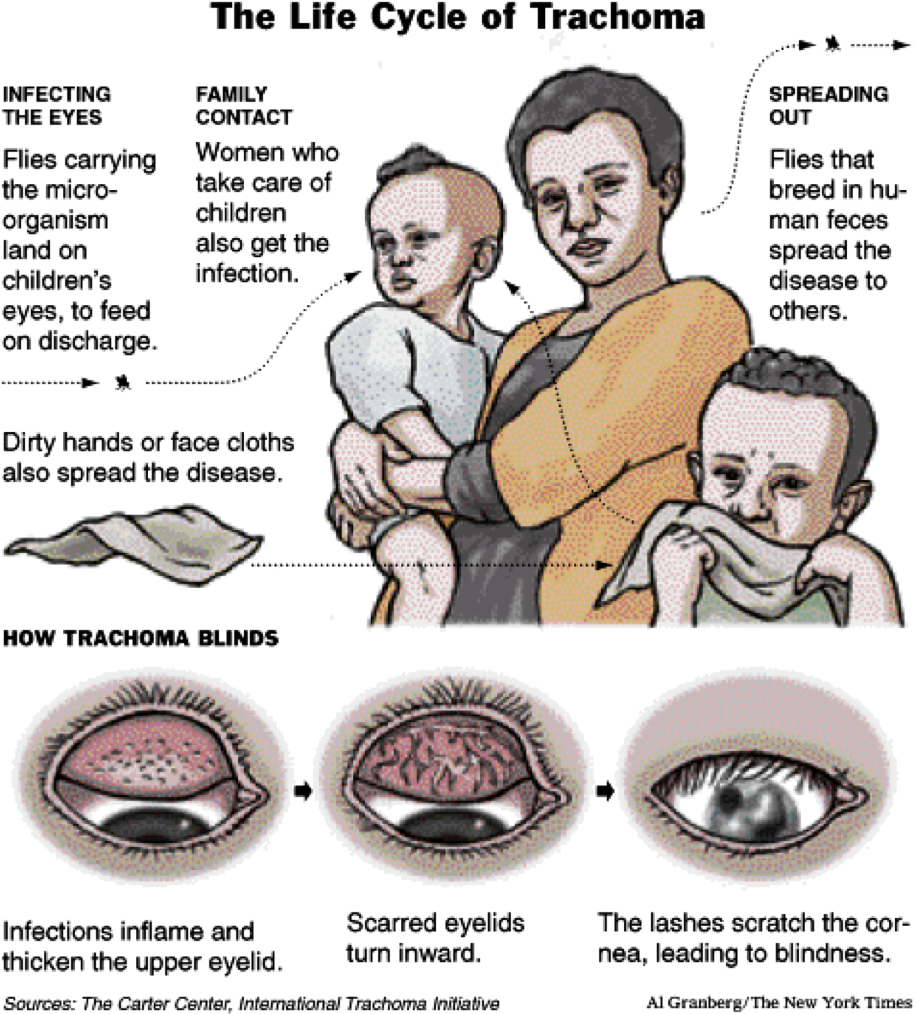
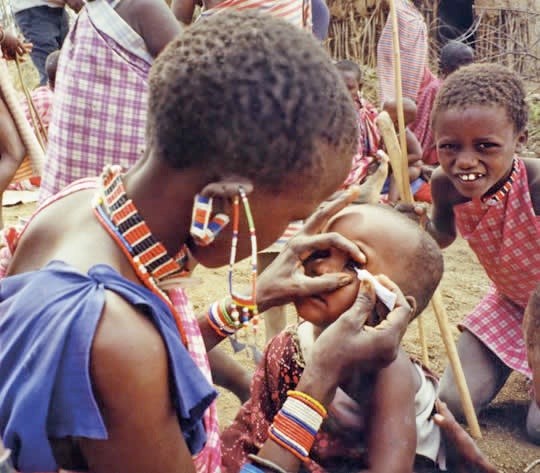
In de vroege stadia is trachoom besmettelijk en kan het door oog-handcontact, door bepaalde vliegen of door besmette handdoeken, zakdoeken, oogmake-up en dergelijke worden overgebracht.
Symptomen
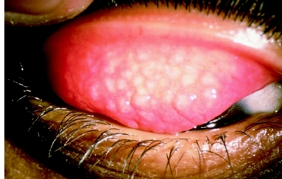
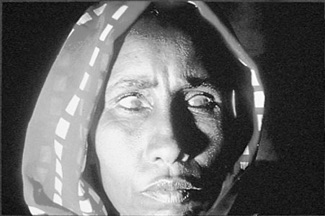
Trachoom tast meestal beide ogen aan. De bindvliezen raken ontstoken, rood en geïrriteerd en de ogen scheiden veel vocht af. Sommige patiënten zijn gevoelig voor fel licht. In de latere stadia groeien er geleidelijk bloedvaten op het hoornvlies (neovascularisatie), wat het zicht belemmert.
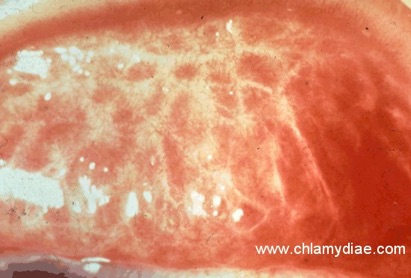
Bij sommige patiënten ontstaat er littekenweefsel op het ooglid, zodat de wimpers naar binnen worden getrokken (trichiasis). Als de patiënt knippert, schuren de wimpers over het hoornvlies, waardoor ze infectie en blijvende schade veroorzaken. Een verminderd gezichtsvermogen of blindheid treedt op bij ongeveer 5% van de mensen met trachoom.
Diagnose en behandeling
Een arts vermoedt trachoom op grond van het uiterlijk van de ogen en de duur van de symptomen. De diagnose kan worden bevestigd indien onderzoek van een oogmonster in een laboratorium uitwijst welk organisme de infectie veroorzaakt.
De behandeling bestaat uit orale toediening van het antibioticum erytromycine of een tetracycline gedurende drie tot vijf weken. Het nieuwere antibioticum azitromycine kan eens per week gedurende één tot drie weken worden gebruikt.
Oogzalven met tetracycline of erytromycine zijn effectief, maar moeten gedurende vier tot zes weken worden aangebracht. Als de aandoening het ooglid, het bindvlies of het hoornvlies beschadigt, kan chirurgisch ingrijpen noodzakelijk zijn.
Omdat de ziekte besmettelijk is, treedt herinfectie vaak op. Regelmatig de handen en het gezicht wassen helpt het verspreiden van de infectie te voorkomen. Artsen dienen vaak antibiotica toe aan hele buurten waar veel mensen aan trachoom lijden.
Young children are particularly susceptible to infection, but the disease progresses slowly, and the more painful symptoms may not emerge until adulthood.
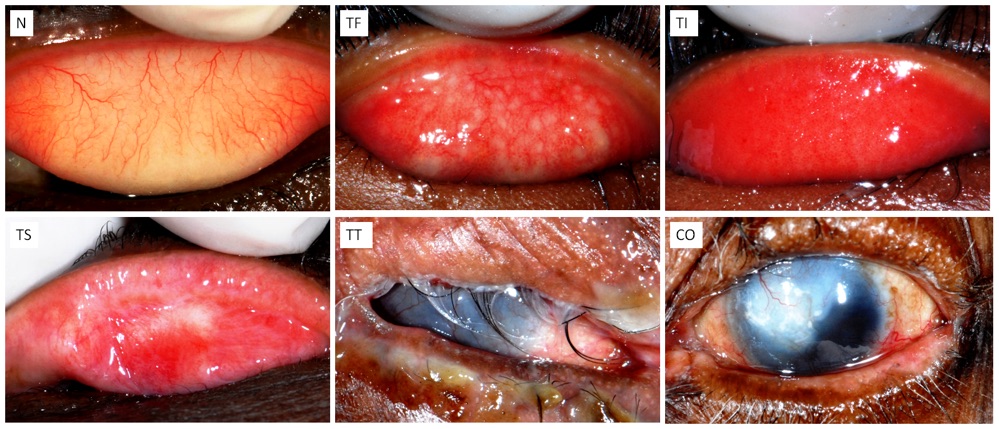
The World Health Organization has identified a grading system with five stages in the development of trachoma. The stages are
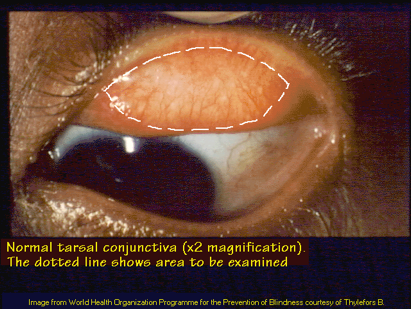
•Inflammation — follicular. The infection is just beginning. Five or more follicles — small bumps that contain lymphocytes, a type of white blood cell — are visible with magnification on the inner surface of the upper eyelid (conjunctiva).
•Inflammation — intense. In this stage, the eye is now highly infectious and becomes irritated, with a thickening or swelling of the upper eyelid.
•Eyelid scarring. Repeated infections lead to scarring of the inner eyelid; the scars often appear as white lines when examined with magnification. The eyelid may become distorted and may turn in (entropion).
•Trichiasis, or ingrown eyelashes. The scarred inner lining of the eyelid continues to deform, causing the lashes to turn in so that they rub on and scratch the transparent outer surface of the eye (cornea). Only about 1 percent of people with trachoma develop this painful condition.
-
•Corneal clouding. The cornea becomes affected by an inflammation that is most commonly seen under the upper lid. Continual inflammation compounded by scratching from the in-turned lashes leads to clouding of the cornea. Secondary infection can lead to development of ulcers on the cornea and eventually partial or complete blindness.

In addition, the lubricating glandular tissue in the lids — including the tear-producing glands (lacrimal glands) — can be affected. This can lead to extreme dryness, aggravating the problem even more.
When to see a doctor
Call your doctor if you or your child has itching, irritation or discharge from the eyes, especially if you recently traveled to an area where trachoma is common.
The principal signs and symptoms in the early stages of trachoma include:
Mild itching and irritation of the eye
Discharge from the eye containing mucus or pus
As the disease progresses, later trachoma symptoms include:
Marked light sensitivity (photophobia)
Blurred vision
Eye pain


The cause of trachoma is certain subtypes of Chlamydia trachomatis, a bacterium that can also cause the sexually transmitted disease chlamydia.
Trachoma spreads through contact with discharge from the eyes or nose of an infected person. Hands, clothing, towels and insects can all be routes for transmission. In the world's developing countries, flies are a major means of transmission.



Factors that increase your risk of contracting trachoma include:
•Poverty. Trachoma is primarily a disease of extremely poor populations.
•Crowded living conditions. Families living in close contact are at greater risk of spreading infection.
•Poor sanitation. Poor hygienic conditions facilitate spread of the disease.
•Age. In areas where the disease is endemic, it's most common in children ages 3 to 5.
•Sex. Women contract the disease at higher rates than men do. Women are also blinded up to four times more often than men are.
•Poor access to water. Households at greater distances from a water supply are more susceptible to infection.
•Flies. People living in areas with problems controlling the fly population may be more susceptible.
•Lack of latrines. Populations without access to working latrines have a higher incidence of the disease.










One episode of infection with Chlamydia trachomatis is easily treated with early detection and use of antibiotics. However, repeated infection can lead to complications, including:
•Scarring of the inner eyelid
•Eyelid deformities
•Inward folding of the eyelid (entropion)
•Ingrown eyelashes
•Corneal scarring or cloudiness
•Partial or complete vision loss


Symptomen
Oorzaak
Risicofactoren
Complicaties
Trachoma treatment options depend on the stage of development.
Medications
In the early stages of trachoma, treatment with antibiotics alone may be enough to eliminate the infection. The two drugs currently in use include a tetracycline eye ointment and oral azithromycin (Zithromax). Although azithromycin appears to be more effective than tetracycline, azithromycin is more expensive. In poor communities, the drug used often depends on which one is available and affordable.

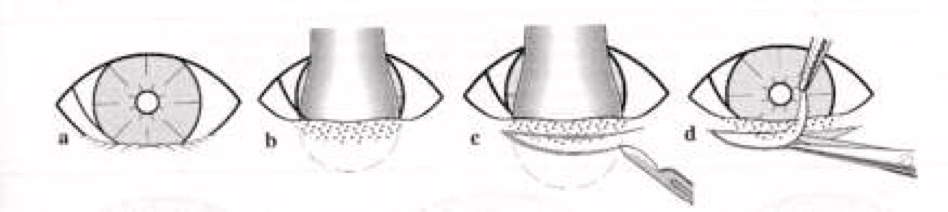
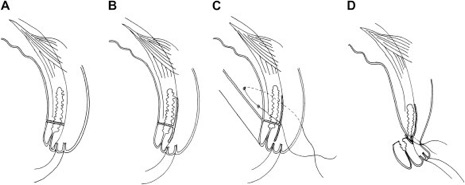
Treatment of later stages of trachoma — including painful eyelid deformities — may require surgery.
In eyelid rotation surgery (bilamellar tarsal rotation), a doctor makes an incision in the scarred lid and rotates the eyelashes away from the cornea. The procedure limits the progression of corneal scarring and can improve eyesight. Generally, this procedure can be performed on an outpatient basis.
The procedure takes less than 15 minutes and has a good long-term success rate.If the cornea has become clouded enough to seriously impair vision, corneal transplantation is an option that offers some hope of improved vision; frequently, however, the results are not good.

Behandeling



Amsterdam Eye Hospital
Oogziekenhuis Amsterdam